Long decried and controversy, the laser gradually takes its place in endodontics, and especially the Erbium EAG which meets the requirements and objectives of irrigation, endodontic disinfection, root canal system, isthmus and dentinal tubules. The exacerbation of the irrigation dynamics will allow to transport the irrigant to the foramen. Ensuring its disinfection and meeting the objectives of modern endodontics. This will upset our concepts of "over preparation" too often anchored and meet the criteria of tissue saving. Indeed, there is no need to over-instrument a canal to ensure its cleaning; (Fig. 1).
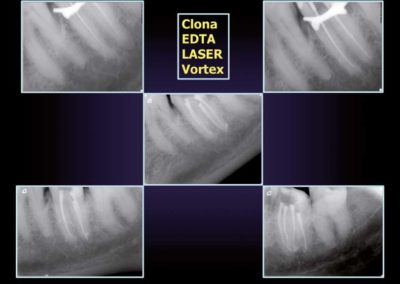
The use of titanium nickel instruments, such as the Vortex (Dentsply), which, like Profile (Dentsply), optimizes the rise of debris is part of this new philosophy. In fact the combination of the rising of debris and irrigation potentiated by the laser Erb Yag Syneron will allow us an optimized cleaning, with a ductal preparation at minima, therefore not mutilating.
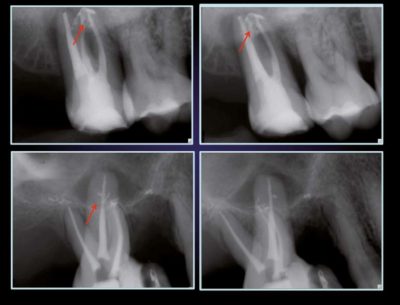
All that remains is to seal with a Thermafil technique, which does not require instrumentation to transport and compact hot gutta into the last tenths foraminous millimeter. Thus it' s possible to combine optimal cleaning and compacting; (Fig. 2) in the foraminous areas, and even to block inter-canal isthmus. This is particularly obvious on the third image: (Fig. 3) which shows the difference between two completely opposite endodontics.

The initial radiograph revealed a radiographically correct endodontic treatment ; however the retreatment and laser irrigation shows us two different "endodontic worlds". It is then possible to see at the time of the filling the non-instrumented areas which have been cleaned and sealed. This is also the case for the mandibular molars; (Fig. 4) which very frequently present complex root canal anatomies. It is even possible to speak of mesial canal system, with the presence as in this clinical case of three distinct canals.
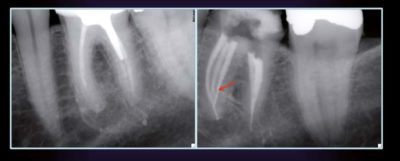
But that this mesial root of the mandibular molars contains one, two, three canals, they will always be connected by isthmus. And this is where the notion of instrumented and non-instrumented zones takes on its importance. In fact, these canals are connected by isthmic systems which harbor a more or less pathogenic bacterial fiber, taking the key role of sword of Damocles, with obviously the possibility of progressive colonization of the untreated root canal system. This can explain lesions evolving lately, with the progressive introduction of lesions of endodontic origin, sometimes voluminous (Cochet / Khayat, 2012).
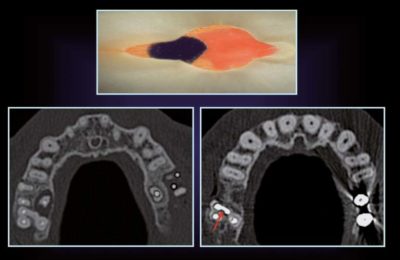
Chronic maxillary sinusitis
In the maxillary, the problem is medically quickly more annoying. The bacterial diffusion at the level of the maxillary molars is at the origin of a large number of chronic sinusitis. They are mainly caused by the non-treatment of the MB2 and exist, unfortunately, in more than 90% of the cases.
They can also be developed from isthmic systems as in the present case; (Fig. 5). A "classical" anatomy with 4 canals (MB1, MB2, DV and P) can be observed at the level of the 26th. Its inadequate endodontic treatment shows us the establishment of a lesion.
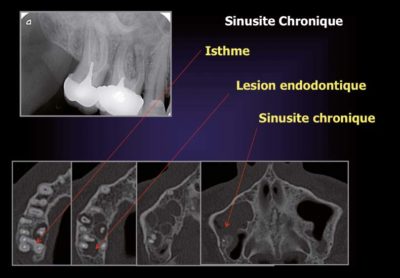
Radiography is very far from the clinical reality (Roisin / Chausson / Cochet: 2000 - 2001). The CBCT or the scanner will show us a much more complex anatomy than it appeared radiographically. Lesions that were not visible on the radios, and of course a sinusian pathology not visible and suspected radio graphically (Roisin / Chausson / Cochet 2000.2001).
But in order to solve the medical and sinus problem, it is necessary to have an effective endodontic treatment to obtain the healing of the lesions of endodontic origin, and succeed to treat these isthmic far from the distance of the main canals. Thus, we have the proof of the importance of the assisted irrigation laser.
We can see that the canal anatomy has been completely cleansed.
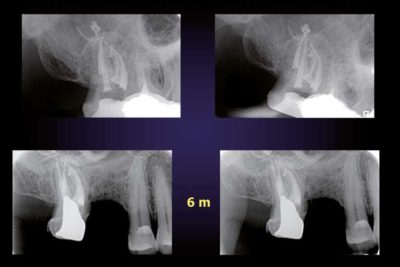
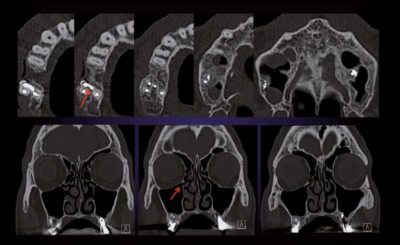
The end-of-treatment radiography and its 6-month follow-up; (Fig. 6) demonstrate good clinical stability, but only the CBCT will give us real information; (Fig. 7). It is possible to see how rich it is with information. We can see that the root canal anatomy has been completely cleansed, that the lesions of endodontic origin are regenerated and that the sinus pathology has disappeared. The coronal sections even show a perfect aeration of the sinus, so the medical problem is solved.(Cochet, 2012).
It is therefore proven that this healing requires appropriate endodontic treatment. This requires a thorough cleaning of the canal system, isthmus and non-instrumented areas inaccessible to endodontic instruments, it is the only guarantee of treatment, (Cochet, 2012).A hermetic and compressive sealing to fill the non-instrumented areas is essential; (Fig. 8) with possibly the combination of traditional gutta cones and Thermafil, as shown in this section. This will ensure the serenity of our endodontic treatments by avoiding secondary bacterial recolonization.